



 DIAMOND tarso-conjunctival excision (medial conjunctivo-plasty)
DIAMOND tarso-conjunctival excision (medial conjunctivo-plasty) 1. Place probe in inferior canaliculus
2. Evert lower lid
3. Excise a diamond of tarsoconjunctival immediately below the punctum
4. Vircyl 5-0 double arm
through conj below apex of diamond immediately below punctum
apposing NORTH & SOUTH corners of diamond
lower lid retractor should be included in the suturee
to prevent punctum fr pouting outward on downgaze
overall effects
tightening of lowerlid retraction
invert the punctum
 Lazy T procedure (DIAMOND + BICK-medial)
Lazy T procedure (DIAMOND + BICK-medial) medial conjunctivo-plasty + full thickness PENTAGON lid excision
1. Full thickness PENTAGON Lid excision
2. DIAMOND tarso-conjunctival excision
3. Opposition of full thickness PENTAGON lid excision wound
Lazy T- look like letter T lying down resting
 Plication of ANTERIOR limb of tendon
Plication of ANTERIOR limb of tendon 1. Lower canaliculus held taut against globe with lacrimal probe
2. Horizontal skin incision- placed just below lower canaliculus
3. Incision extends fr just lateral to punctum
(permit exposure of medial edge of tarsal plate)
to just medial to medial canthal corner
4. Anterior limb of medial canthal tendon identified & exposed
5. Non-absorbable suture passed thro medial end of tarsus
just below level of punctum & thro medial canthal tendon
in a position superior & posterior to tarsal stitch
6. Suture tied tight enough to overcome medial laxity
not too tight to cause punctal eversion
postero-superior position of medial end of stitch
important to avoid ant displaceM of whole medial canthal corner
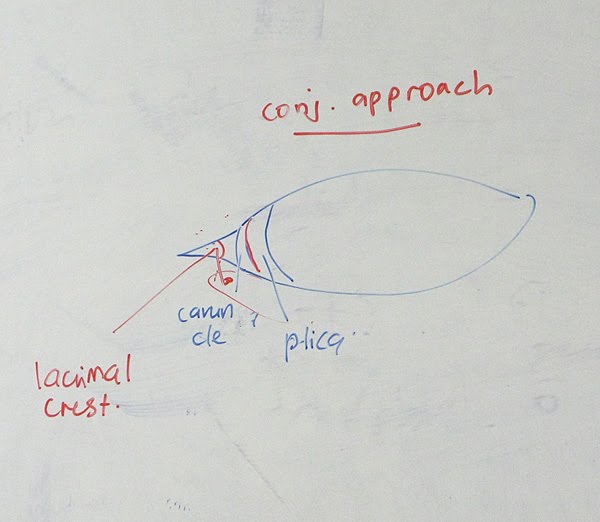 Plication of POSTERIOR limb of tendon
Plication of POSTERIOR limb of tendon 1. Conjunctival incision mede in fold behind caruncle
2. Incision extend anteriorly to medial end of tarsal plate
3. Lacrimal probe placed in lower canaliculus to indicate position of lacrimal sac
help identify posterior lacrimal crest
4. Posterior lacrimal crest exposed
to allow fixation of one end of non-absorbable suture
5. The other end is secured in posterior surface of the medial end of the tarsus
close to its superior border
6. Knot is buried and the conjunctiva closed.



Bick's procedure
1. Pentagon full thickness lid margin excision
5 mm fr lateral canthus
2. Oppose both cut end

Kuhnt Szymanowski
"1. Skin flap incision from 1/3 medial to lateral, 2 mm below lid margin"
2. Bick procedure
3. Close skin flap & excise excess skin
* Lateral Cantal Tendon Laxity Only -> Lateral Tarsal Strip
 Lateral Tarsal strip
Lateral Tarsal strip 1. Lateral canthal laxity- a/w tarsal sag & poor snap back response
Procedure
1. Cantholysis of inferior lateral canthal tendon
Lateral canthal corner- opened w horizontal incision
Inferior limb of lateral canthal tendon exposed & divided
2. Medial end of the wound lifted upward & laterally
to overlap surgical site
& determine how much horizontal shortening required
3. Strip fashioned by clearing it of
skin & orbicularis anteriorly
Lash margin superior
conjunctiva posteriorly
4. Newly fashioned strip- attach w non-absorbable suture to periosteum
just inside lateral orbital rim at mid pupillary level
which places it just under upper limb of lateral canthal tendon
------------------
CICATRICIAL ECTROPION


Z-plasty
1. Central limb of Z- placed along line of scar
2. Limbs are equal in length
3. Optimal angle btwn limb= 60 degree
Z-plasty produce gain in length along the common limb of original Z
1. Central limb of Z- placed along line of scar
2. Limbs are equal in length
3. Optimal angle btwn limb= 60 degree
Z-plasty produce gain in length along the common limb of original Z
 Skin graft
Skin graft Sources
upper lid- if there is dermatochalasis
pre- or postauricular skin
supraclavicular area
Place compressive bolster over graft-
to enhance graft survival & decrease hematoma formation
The bolster is left for 5 days.
Superior traction suture decreases the risk of recurrent cicatrix postOp



















very informative , thanks a lot
ReplyDelete